The puzzle of consciousness is so devilish that scientists and philosophers are still struggling with how to talk about it, let alone figure out what it is and where it comes from.
The puzzle of consciousness is so devilish that scientists and philosophers are still struggling with how to talk about it, let alone figure out what it is and where it comes from.
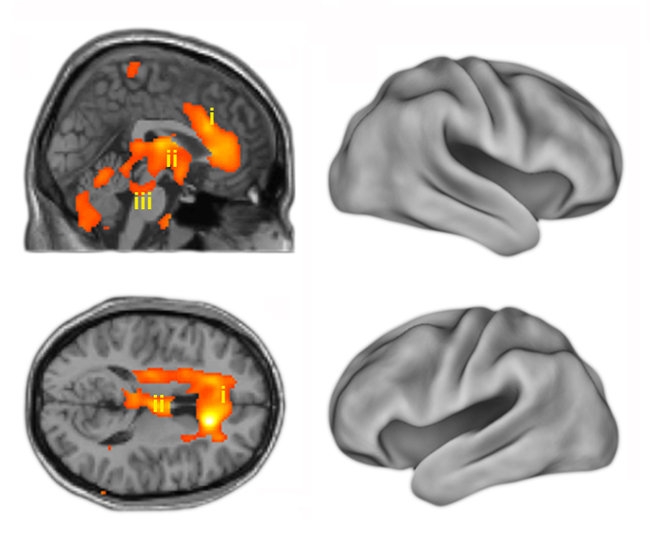 |
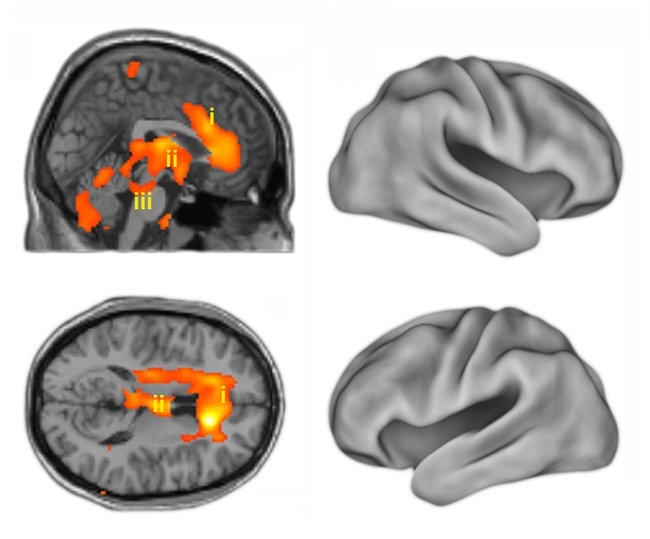
| PET scans show that the return of consciousness after anesthesia involves ancient brain structures that evolved long ago, rather than the more recent neocortex. Side and top down views show activation of the anterior cingulate cortex (i), thalamus (ii) and the brainstem (iii) overlaid on magnetic resonance image slices. |
One problem is that the word has more than one meaning. Trying to plumb the nature of self-awareness or self-consciousness leads down one infamous rabbit hole. But what if the subject is simply the difference in brain activity between being conscious and being unconscious?
Scientists and doctors certainly know how to knock people out. Michael T. Alkire at the University of California, Irvine, put it this way in an article in Science in 2008: “How consciousness arises in the brain remains unknown,” he wrote. “Yet, for nearly two centuries our ignorance has not hampered the use of general anesthesia for routinely extinguishing consciousness during surgery.” And a good thing, too.
Setting aside what philosophers call “the hard problem” (self-awareness), a lot has been learned about the boundary between being awake and alert and being unconscious since ether was used in 1846 to put a patient under for surgery. Researchers have used anesthesia, recently in combination with brain scans, as a tool to see what happens in the brain when people fade in and out of consciousness — which parts turn on and which turn off.
For instance, in a recent study, investigators showed that a person could respond to a simple command to open his eyes (the subjects were all right-handed men) when the higher parts of the brain were not yet turned on. The finding may be useful in deciding how to measure the effects of anesthetics, and it adds another data point to knowledge of what’s going on in the brain.
As in previous studies, the researchers, led by Harry Scheinin and Jaakko W. Langsjo of the University of Turku, in Finland, and Dr. Alkire found that the brainstem and other primitive parts of the brain, like the thalamus, wake up first. The neocortex, the part where all the complicated thinking goes on, wakes up later.
Earlier research has also suggested that consciousness is not a simple state that is either on or off. There are gradations. And there are distinctions that are not immediately obvious, such as the difference between being unresponsive and being unconscious. In 2006, for example, Adrian M. Owen, of Cambridge University in England, reported in the journal Science that a patient who was apparently in a vegetative state showed signs of conscious activity in her brain when asked to imagine playing tennis and other movement.
The finding contributed to disputes over how to treat such patients. It came shortly after a court battle over removing a feeding tube from Terri Schiavo, a Florida woman in a vegetative state. Her husband, who prevailed, argued that she would not have wanted extreme measures to continue.
In studies using anesthesia, the paralytic effects of drugs used during surgery were blocked from one forearm, and then attempts were made to communicate with the patient. Dr. Alkire wrote, “Patients under general anesthesia can sometimes carry on a conversation using hand signals, but postoperatively, they deny ever being awake. Thus, retrospective oblivion is no proof of unconsciousness.”
The recent research by Dr. Scheinin and Dr. Langsjo and colleagues, including Dr. Alkire, looked for proof of consciousness. The researchers used brain scans in combination with two drugs, propofol, which helped cause the death of Michael Jackson, and another anesthetic drug, the many-syllabled dexmedetomidine.
The standard measure of unconsciousness is that a subject or patient does not respond to commands. By that standard, when a subject responds, he’s conscious. What makes dexmedetomidine an ideal drug is that people who are completely under can be brought back from oblivion by gentle shaking and loud speaking, even if they are still on the regular dose of the anesthetic.
In Dr. Scheinin’s study, when unconscious subjects on this drug were told to open their eyes, they responded. Then most of them drifted back into apparent unconsciousness, without their brain’s neocortex turning on. Only the brainstem, the thalamus and one part of the cortex were active.
The subjects under propofol were not woken up, but as the drug was withdrawn, the pattern of their awakening fit well with the other data.
Questions remain. What level of consciousness exists without the neocortex? Does this mean the subjects understood what was happening with more primitive brain regions?
And in the broad view, there’s that problem of memory that Dr. Alkire wrote about. If a patient is conscious during surgery but doesn’t remember any of it, is that good enough? It’s a bit like the tree falling in the forest with nobody to hear it. An anesthesiologist’s koan. If even the patient has no recollection of surgery, was he aware?
And how could we possibly know?
(Source: NYTimes)




